215 minutes of person-centred care without going broke - you can do it

The 1 October mandate of 215 direct care minutes aims to improve resident outcomes and ensure providers spend AN-ACC subsidies on care rather than using them to cross-subsidise deficits in hospitality services and/or accommodation.
As subsidy levels will be calibrated to the mandated care minutes, providers will need to implement a demand-based workforce model. These models align care delivery with the resident’s needs and preferences, similar to the way the home care subsidy system works.
A demand-based workforce model emphasises a person-centred approach that focuses on resident needs, choices and desires that must be calibrated to their assessed level of acuity and care needs. Because providers have to use the mandated level of care minutes, there is no “fat” in the system. This also means that the provider does not set the care agenda. As residents become more aware of the care minutes requirement, we expect they will increasingly ask, “Am I getting my 215 direct care minutes?” We see this approach as supporting resident autonomy and promoting supported living rather than simply offering care.
The Financial Challenge and Need for Redesign
While many providers are concerned that these requirements will exacerbate their financial difficulties, government models suggest that only 75% of AN-ACC funding is needed to meet the mandated care minutes.
If this is correct, then you might be tempted to simply add more direct care workers, assuming you can find them. As we show in this Insight, this isn't a feasible solution.
In our experience, providing 215 care minutes at a sustainable cost requires a redesign of the service delivery models. We also see this as an opportunity to transition to a contemporary Wellness and Reablement model that aligns with a person-centred approach.
In this Insight, we share four learnings from our experiences in working with clients to rethink their resource allocation and redesign their rosters.
1. Who to allocate to the task of delivering services
This is crucial to developing a financially viable service model that meets community expectations. The recent Fair Work Commission work value case resulted in higher wages for direct care workers. This elevates the importance of ensuring that direct care workers are not diverted to non-care tasks.
2. What not to have a Registered Nurse do
Making early morning calls to replace staff is not a care function – it is inefficient and often leads to increased agency costs. Consider what happens when RNs get a call at the end of their shift that someone has rung in sick. Their path of least resistance is to call an agency so they can prioritise resident care.
3. Pursue productivity gains
According to the StewartBrown survey, first-quartile homes have increased direct care minutes by 18%, with only an 8% increase in overall staffing minutes. This has been achieved on the back of increased productivity levels in the following areas:
- Care Management: 53% reduction
- Allied Health: 12% reduction
- Lifestyle Services: 43% reduction
- Hotel Services: 6% reduction
- Administration: 10% reduction
4. Better utilisation of non-care workers
While some of the above reductions are achieved through technology and other efficiencies, many improvements involve better utilisation of non-care workers. The 24% increase in laundry hours is one example, which was achieved by having laundry staff return clean clothing to residents instead of care workers.
In another example, a client reduced catering hours by 40% by moving to a kitchen-plated model similar to that used in hotels instead of serveries.
We have also seen catering staff replenishing resident water jugs instead of care workers.
The Fundamentals
Implementing a person-centred model involves a more targeted and efficient use of resources, which is different to the historical nursing model.
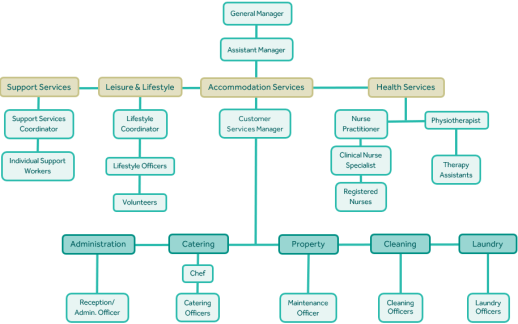
We recommend that providers develop a person-centred model where allied health and nursing are grouped together as health services, combined with a new support stream that includes carers and/or support workers, with both of these teams being overseen by an experienced Wellness & Reablement professional. Typically, we see this person being an Occupational Therapist (O.T).
The following facility staffing model provides a graphic of how this works in practice:
So, how do you do it?
At a task level, it’s really pretty simple. Just follow these four steps:
- Review tasks completed by direct care workers.
- Consider who is the best person for these tasks.
- Redesign workflows to create efficiencies and reduce costs.
- Hold some meetings and roll out the new model.
If it's that simple, what can go wrong? - EVERYTHING
There are two truisms about staff:
- They like the way things are, otherwise, they wouldn’t be the way they are, and
- Humans are hard-wired against change.
How we help
It’s not about knowing what has to be done; it’s about knowing how to do it and having credibility when you ask people to step outside of their comfort zones.
Often, having an independent recognised expert is the key to success. They can validate the proposed changes on the basis that “we’ve done this with many providers”. They also take away the “you’re only doing this to make more money” argument. Because they bring objectivity and experience to the process, they should be able to pace out objections and coach staff through the changes required.
We’ve worked with many providers to help them develop sustainable rosters that meet compliance with care minutes while maintaining or enhancing financial viability. In our experience, unless the provider has someone with a black belt in operational change management, most initiatives fail. By comparison, where we’ve been engaged to oversee the change, while it’s not pain-free, the pain is well managed, and the patient (staff) makes a full recovery!
If you’re experiencing anxiety about the impact of the October care minute increase, give us a call. We’re happy to share some experiences. If you need more assistance, we can support you with our Sustainable Human Resources service.
As a former nurse, facility manager and CEO with a passion for rostering, we welcome your enquiry.
For optimised care minutes and a person-centred model, contact James.
James Saunders
02 9068 0777
james.saunders@prideagedliving.com.au
